The summary section allows to see, in one glance, the key features of a diagnosis
Gender :
all
Age :
5 year (Min), 50 year (Max), 20 year (Mean)
Osteoid osteoma
The osteoid osteoma is very painful benign tumor in young, consisting of a nidus osteogenic not exceeding 15 mm (beyond what is osteoblastoma) and surrounded by a condensation reaction and severe swelling.
- Diaphyseal and metaphyseal (85%), epiphyseal (15%)
- Cortical (80%) or subperiosteal (20%), rarely spongy
Clinic:
- Typical form: schedule inflammatory pain (except at the beginning of evolution), to increase night, calmed by aspirin and NSAIDs such as those blocking the way of cox 2.
- A hip may simulate hip disease, particularly in children, or occur only by knee pain.
Think osteoid osteoma of the hip or femoral shaft to unexplained knee pain in children especially if the schedule is inflammatory
- Constant atrophy in the shapes of members
X-rays:
- They may be normal. They may show hyperostosis or unilamellar periosteal reaction continues.
- The nidus itself is rarely visible on radiographs.
CT:
- Nidus (tumor itself):
bone gap of 5 to 15 mm at regular edges. The three key signs on CT:
1 the nidus is generally round or oval on an axial section. 3D, it may be slightly elongated along the major axis of the bone, but its greatest diameter never exceed 2.5 times the smallest diameter.
2 In 85% of cases, the nidus has a central calcification, punctate, arcuate or nodular.
3 Even when calcification is important, there is still a clear border between the circumferential calcification and peripheral condensation.
- Surrounded by a gradually decreasing to normal bone condensation (condensation inflammatory).
- Compact periosteal reaction (thickening of the cortex) or unilamellar can continue
MRI:
- Nidus hypointense signal on T2 and T1 with contrast (except calcification)
- The nidus is the contrast from the arterial phase of the dynamic sequence after injection.
- Edema of the spongy and soft tissue very important when it is desired sequence spread a false image or osteitis
- Synovitis (synovial thickening and effusion) in the epiphyseal forms.
Bone scan:
- The uptake by the vascular phase and three time with typically a very small central focus hyperfixant (nidus) surrounded by a less intense halo (reaction device). - Supplanted by MRI with injection and dynamic sequence.
Treatment:
- Destruction percutaneous laser photocoagulation or radiofrequency electrocoagulation. Recurrence rate of 3% entrained hands
- The indications for surgical excision is reserved for cases where the percutaneous treatment is impossible, certain tumors of the posterior arch of the vertebrae.
Differential Diagnoses:
- False images nidus (irregular bone texture, vascular channel ...).
- Brodie abscess (infection context, elongated or sinusoidal receiver lying)
Review key dynamic MRI sequence after injection: the nidus of osteoid osteoma is the contrast from the arterial phase while most other diseases take the contrast so delayed and progressive
- Osteoblastoma: very close picture but multiple punctate calcifications, lobed edges, seat subchondral willingly bearing zone which is rare for osteoid osteoma
Case
Osteoid osteoma of the medial cortex of the femoral neck (the most common location). Thickening of the medial cortex of the femoral neck containing a clear, better seen on CT image corresponding to the nidus (arrow).
The axial section of the scanner (C), the nidus (thin arrow) is surrounded by a net condensation on the inner side and fuzzy to normal bone (thick arrows).
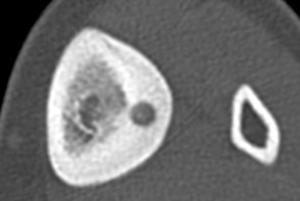
03: cortical osteoid osteoma of the tibia. Note the very discrete calcification nidus and the importance of cortical thickening [R2]
Osteoid osteoma
The osteoid osteoma is very painful benign tumor in young, consisting of a nidus osteogenic not exceeding 15 mm (beyond what is osteoblastoma) and surrounded by a condensation reaction and severe swelling.
12% of benign bone tumors.
Age: 5-25 years (80%)
Men >> Women (3/1)
Location:
- Femur (30%) (upper end)> Tibia (15%)> spine (posterior arch) (8%)> Hands - Feet


- Diaphyseal and metaphyseal (85%), epiphyseal (15%)
- Cortical (80%) or subperiosteal (20%), rarely spongy
Clinic:
- Typical form: schedule inflammatory pain (except at the beginning of evolution), to increase night, calmed by aspirin and NSAIDs such as those blocking the way of cox 2.
- A hip may simulate hip disease, particularly in children, or occur only by knee pain.
Think osteoid osteoma of the hip or femoral shaft to unexplained knee pain in children especially if the schedule is inflammatory
- Constant atrophy in the shapes of members
X-rays:
- They may be normal. They may show hyperostosis or unilamellar periosteal reaction continues.
- The nidus itself is rarely visible on radiographs.
CT:
- Nidus (tumor itself):
bone gap of 5 to 15 mm at regular edges.
The three key signs on CT:
1 the nidus is generally round or oval on an axial section. 3D, it may be slightly elongated along the major axis of the bone, but its greatest diameter never exceed 2.5 times the smallest diameter.
2 In 85% of cases, the nidus has a central calcification, punctate, arcuate or nodular.
3 Even when calcification is important, there is still a clear border between the circumferential calcification and peripheral condensation.
- Surrounded by a gradually decreasing to normal bone condensation (condensation inflammatory).
- Compact periosteal reaction (thickening of the cortex) or unilamellar can continue
MRI:
- Nidus hypointense signal on T2 and T1 with contrast (except calcification)
- The nidus is the contrast from the arterial phase of the dynamic sequence after injection.
- Edema of the spongy and soft tissue very important when it is desired sequence spread a false image or osteitis
- Synovitis (synovial thickening and effusion) in the epiphyseal forms.
Bone scan:
- The uptake by the vascular phase and three time with typically a very small central focus hyperfixant (nidus) surrounded by a less intense halo (reaction device).
- Supplanted by MRI with injection and dynamic sequence.
Treatment:
- Destruction percutaneous laser photocoagulation or radiofrequency electrocoagulation. Recurrence rate of 3% entrained hands
- The indications for surgical excision is reserved for cases where the percutaneous treatment is impossible, certain tumors of the posterior arch of the vertebrae.
Differential Diagnoses:
- False images nidus (irregular bone texture, vascular channel ...).
- Brodie abscess (infection context, elongated or sinusoidal receiver lying)
Review key dynamic MRI sequence after injection: the nidus of osteoid osteoma is the contrast from the arterial phase while most other diseases take the contrast so delayed and progressive
- Osteoblastoma: very close picture but multiple punctate calcifications, lobed edges, seat subchondral willingly bearing zone which is rare for osteoid osteoma
Case
Osteoid osteoma of the medial cortex of the femoral neck (the most common location). Thickening of the medial cortex of the femoral neck containing a clear, better seen on CT image corresponding to the nidus (arrow).
The axial section of the scanner (C), the nidus (thin arrow) is surrounded by a net condensation on the inner side and fuzzy to normal bone (thick arrows).
03: cortical osteoid osteoma of the tibia. Note the very discrete calcification nidus and the importance of cortical thickening [R2]